Vitamin D: Supplement Review
Vitamin D or ‘D’ as I will refer to it moving forward, plays an active role in immune function, protein synthesis, muscle function, cardiovascular function, cell growth and musculoskeletal regulation…so a lot. Its influence on all of these systems opens the potential for many possible benefits to athletic performance, recovery and injury prevention.
Staying healthy has never been at more of a premium. Sporting rules have changed regarding practicing and playing with flu-like symptoms, during the pandemic. As I write this, sports are currently on hold, but there is hope to see their return in January.
Athletes are constantly pushing their bodies to the brink of exhaustion with training. This combined with poor sleep habits, school or work, and a host of other social stressors creates a perfect storm for getting sick. Traditionally, you may have been able to show up to practice with the sniffles and a cough and gut it out. Now, you are likely to be sitting at home while your peers continue to practice and develop, putting you at risk of losing minutes come game time. Practice minutes are always in short supply so missing valuable reps because of sickness means you’re going to be chasing to catch up once you’re healthy.
Apart from D’s role in immune function by preventing acute upper respiratory tract infections like the common cold and influenza (which have a high incidence in elite athletes), it has been shown to have a positive influence in many other areas. Maintaining bone density to limit the incidence of stress fractures, influencing muscle growth (type II, fast twitch fibres), and performance. There is some evidence to suggest insufficient levels delay recovery after surgery and sufficient levels can accelerate recovery of muscles after intense exercise.
A strong relationship has been established between severe D deficiency and sudden cardiac death, in athletes.
Although many benefits have been noted, there remains significant uncertainty as to what the proper level of D should be, especially in athletes. This means that the dosage one should be supplementing with raises some questions as to what level you are trying to obtain.
The Endocrine Society use the below bolded measures as cut-offs:
>40ng/mL *** [used in some studies of athletes as an ‘ideal’]
>30ng/mL = sufficient
30ng/mL-20ng/mL = insufficient 70% of Americans
<20ng/mL = deficient 29% of Americans
~1000 IU of D will increase your blood level by 5ng/mL
The safe upper limit for D intake is set at 4,000 IU/day. This is what I take.
The best way to find out your baseline is to get a blood test done. This can guide you towards how much you should be supplementing with to have a ‘sufficient’ level.
A study of 2313 athletes found that 56% had inadequate levels of D when using <32ng/mL as a cut off.
As humans, our main source of D production is from the sun (UVB) and takes place in the skin. Thus, anything that blocks our skin will block our D production (clothes, sun screen etc.) We can get some from our diet (certain fish, red meat and a few other sources) but generally at low levels. In the absence of adequate sun exposure to produce D (especially in the northern hemisphere, like us Canadians), our main source must be supplementation. This is even more important if we have any factors that would limit our ability to convert UVB to D. In a young, healthy, athletic group this would be darker skin tone (or a higher level of melanin in the skin). Darker skin tone is an adaptation that is advantageous to prevent burning in hotter, more equatorial environments but still allow for D production due to total exposure throughout the day. People’s with darker skin tone in areas with a low UV index are much more likely to have D insufficiencies.

Lots of blue up north…if we’re lucky we have a UV Index of 1 up in central AB…probably 0.
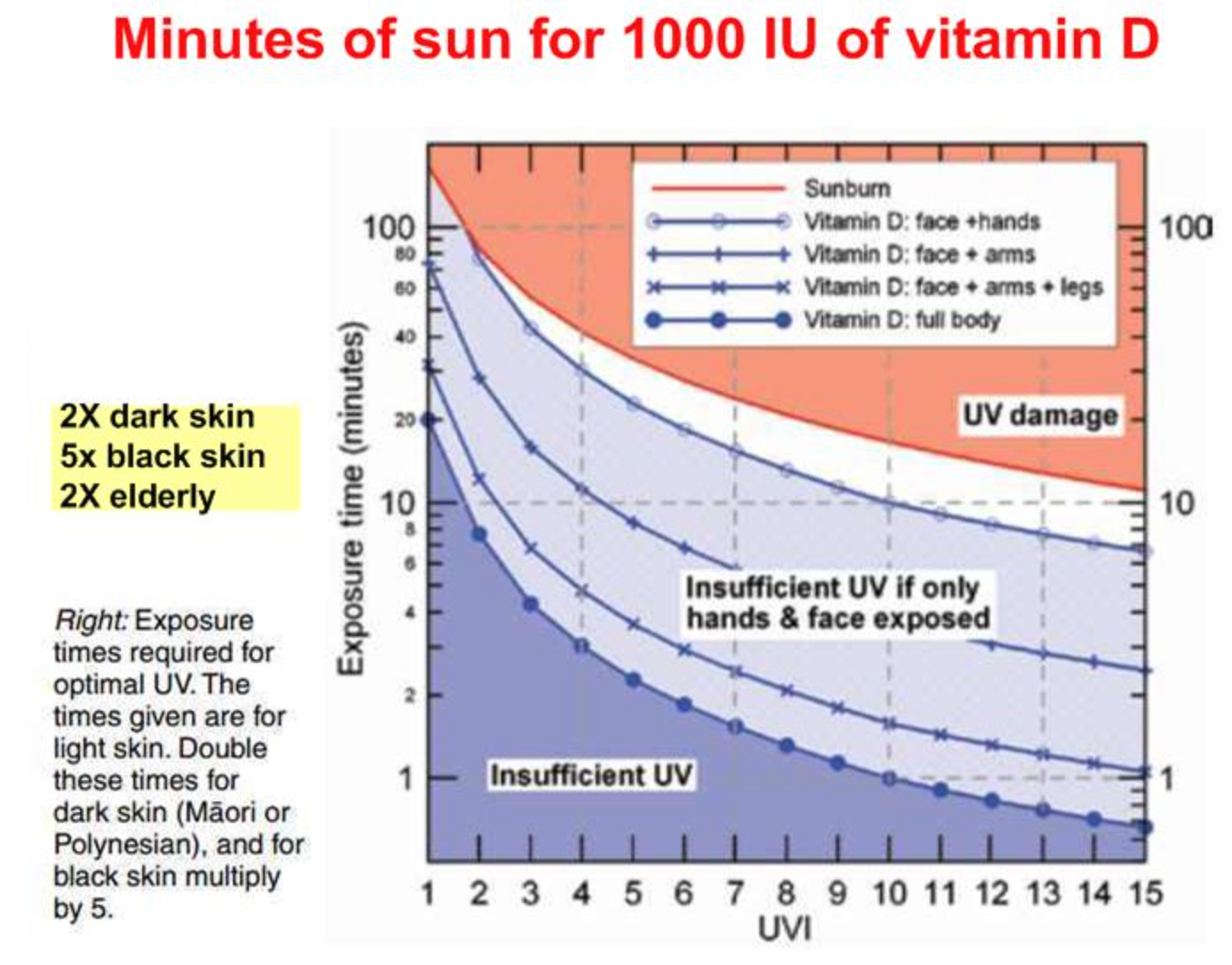
At first glance it looks like you may only need ~20 minutes of sun to get a 5ng/ml bump of D (which may or may not get you to sufficient levels depending on your baseline), however, that 20 minutes is if you’re laying naked outside…and are young…and thin… and have fair skin. Not my preferred choice in the middle of winter. If we look at the graph with clothing on we are now at a minimum of an hour but likely closer to 2 hours. It becomes quite laughable to assume that us Canadian’s can rely on the sun for our daily D re-up, especially in the winter.
https://vitamindwiki.com/No+%E2%80%93+10+minutes+per+day+of+sun-UVB+is+NOT+enough
The pandemic has put numerous stressors on our society but most relevant to this discussion, our physical and physiological health. Shelter-in-place orders, lock downs, and fear of getting COVID have put numerous strains on getting outdoors (to get the D) and remaining active. Not to mention we are now in winter and the weather has been too nice thus far which must mean January and February will be a frozen hell.
At this point in the discussion things get a bit more speculative as we dive into the potential of D supplementation to reduce COVID-19 infection, severity and mortality.
There appears to be, at least, a correlation between D deficiency and those in the hospital/ICU (more severe pathology).
What we know from SARS-COV-1 is that it acts by binding to ACE2 receptors in the lungs, causing a reduction of the receptor, which plays an important role in preventing acute lung damage. Less receptors = more damage. SARS-COV-2 (COVID-19) seems to act in a similar fashion.
D fits in to this equation by increasing ACE2 receptors in conditions where ACE2 receptors are reduced. This helps to reduce the damage done by a low ACE2 receptor environment. Potentially mitigating some of the COVID-19 effects. Interestingly, it doesn’t seem to impact ACE2 receptor levels when the individual is healthy, meaning it seems to act to maintain a homeostasis of the receptor.
None of this is to suggest that D is the golden goose of COVID prevention but it is cheap and available. There is a growing amount of ‘smoke’ in the research and one starts to wonder if the ‘fire’ is near. The additional commentary below dives into this more with a full list of sources.
Suboptimal levels of D seem to increase the risk of respiratory illness (including COVID-19) and stress fractures and effect muscle function and growth.
If you are looking for more information on the topic:
https://www.bmj.com/content/371/bmj.m3872/rr-5 - additional commentary
Episode 1474 JRE with Dr. Rhonda Patrick [10-56min]
https://www.foundmyfitness.com/ - Dr. Rhonda Patrick
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7071499/#B49-nutrients-12-00579 Role of Vitamin D in Athletes and Their Performance: Current Concepts and New Trends
Additional references can be supplied upon request
Disclaimer: Always consult with the appropriate health authority to make sure it’s safe for you to add or change any supplements in your diet.